" transform="translate(5 2)" width="10px"/></svg>)
•
5 min read
How to Simplify Discharge Summary Writing: A Complete Guide for Physicians in March 2026

•
5 min read
How to Simplify Discharge Summary Writing: A Complete Guide for Physicians in March 2026
Physicians often spend 15 to 20 minutes writing each discharge summary, usually hours after rounds when key clinical details are harder to recall. That delay turns a straightforward documentation task into a slow reconstruction of decisions, medications, and follow-up plans from memory. Learning how to streamline discharge summary writing begins with capturing information while patient care is still unfolding and using voice-based documentation that records clinical reasoning at speaking speed. Instead of typing summaries long after discharge, clinicians can speak their hospital course and care plan while details are still fresh, turning real-time explanations into structured documentation inside the EHR with modern dictation software.
TLDR:
Delayed discharge summaries increase 30-day readmissions by 1.60% per day of delay.
Speaking reaches 120-150 words per minute versus 40 typing, cutting documentation time by 3-4x.
Complete summaries during rounds when clinical details are fresh, not hours later.
Templates and auto-populated EHR fields remove repetitive data entry from discharge summaries.
Some modern tools learn your medical vocabulary with 200ms speed and HIPAA compliance for team-wide documentation.
Why Discharge Summary Speed Matters for Patient Safety and Care Transitions
Discharge summaries go beyond documentation. When these documents are delayed or incomplete, patients face real risks during care transitions.
The numbers tell a concerning story. Research shows that 37.6% of discharge summaries are released at least one day after patients leave the hospital. For every day of delay, the likelihood of 30-day hospital readmission increases by 1.60%. Longer delays in completing discharge summaries are associated with higher rates of 30-day readmission in some studies.
These delays create dangerous information gaps. Primary care physicians receiving patients may lack critical details about medications changed during hospitalization, pending test results, or necessary follow-up appointments. Without this information, care coordination breaks down.
The consequences extend beyond readmissions. Incomplete summaries contribute to medication errors, duplicated tests, and missed diagnoses. When your next provider doesn't know what happened during your hospital stay, they're working blind.
Faster completion isn't about checking boxes. In the days following discharge, when patients are particularly vulnerable to complications, a complete summary can help prevent emergency visits and catch issues early.
The True Cost of Documentation Burden on Physicians
Documentation drains more than time. Physicians spend 15.5 hours weekly on paperwork and admin tasks, according to the 2023 Medscape Physician Compensation Report. Reducing documentation time becomes critical as these hours add up. That translates to nearly two full workdays diverted from patient care.
Those hours add up fast. At four patients per hour, 15.5 hours of admin work means 62 patients you could have seen each week. Over a year, that's more than 3,000 missed appointments per physician.
For physicians who could otherwise see patients during that time, administrative work represents a substantial opportunity cost in both patient access and clinical productivity. But the real toll isn't financial. Burnout rates climb as documentation demands grow. Time spent writing discharge summaries late at night is time away from family, sleep, and recovery.
You didn't train for a decade to become a data entry specialist.
Critical Components of an Effective Discharge Summary
Every discharge summary needs specific elements to meet Joint Commission standards and protect patients during transitions. The goal is completeness without bloat.
Patient Demographics and Admission Details
Start with the basics: patient name, medical record number, admission date, discharge date, and attending physician. Include the primary admission diagnosis and any secondary diagnoses that shaped the hospital course. Medical summaries require precision and completeness. These identifiers prevent confusion when multiple providers review the record.
Hospital Course Narrative
Summarize what happened during the stay in chronological order. Focus on clinical decision-making, procedures performed, and how the patient responded to treatment. Skip routine vital sign trends unless they informed major clinical decisions. This section answers: why did this patient need hospitalization, and what changed?
Medication Reconciliation
List all discharge medications with dosages, frequencies, and duration. The ability to speak medical terms without errors prevents dangerous transcription mistakes. Flag any changes from pre-admission medications. Note what was stopped, started, or adjusted. This prevents dangerous drug interactions and duplicate prescriptions.
Follow-Up and Pending Results
Specify which provider should see the patient, when, and why. Document any lab results or imaging studies still pending at discharge. Without this, critical findings fall through the cracks.
Workflow Optimization Strategies to Reduce Completion Time
Small process changes create big time savings. Quality improvement initiatives have reduced discharge summary completion time by 70%, dropping from 71.5 hours to just 21.8 hours. The secret isn't working harder, but restructuring when and how you document.
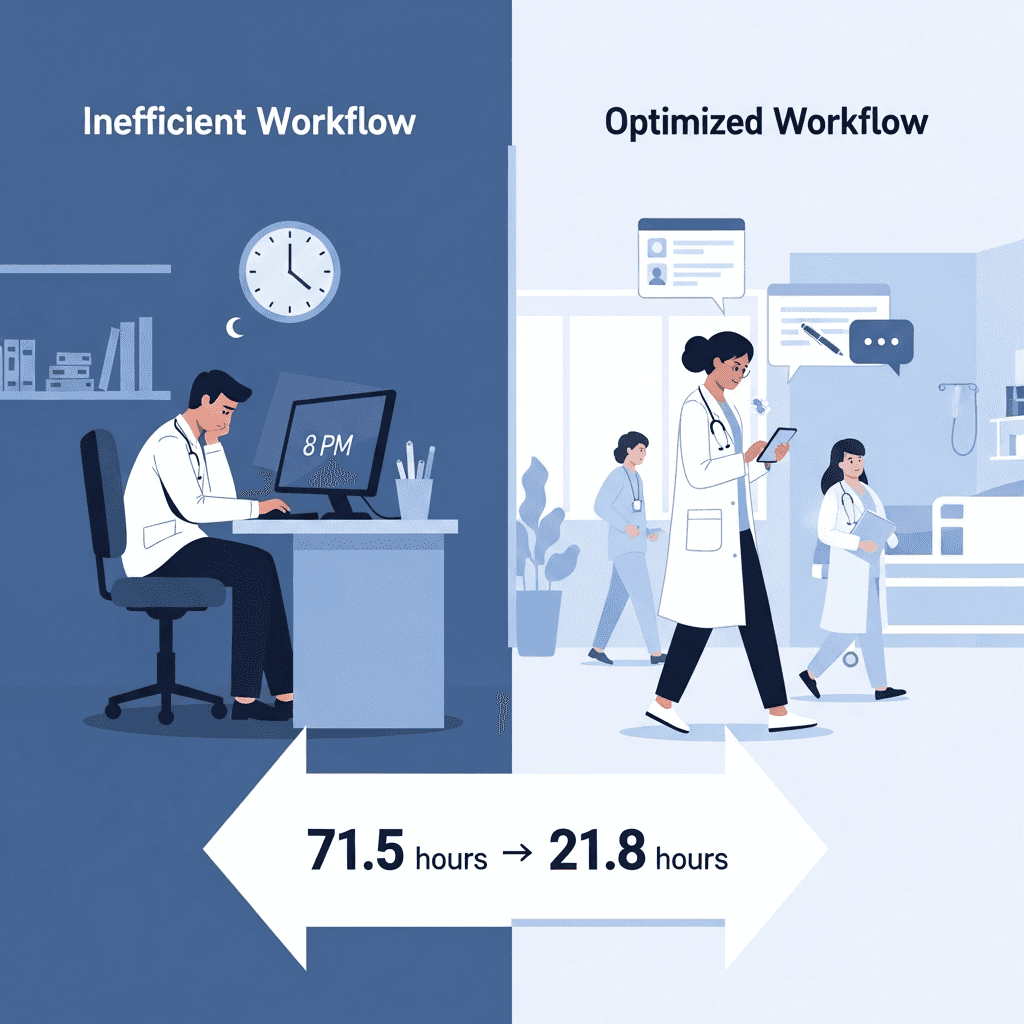
The most effective change? Complete summaries during rounds instead of after your shift ends, using professional dictation software to capture information in real time. When you're at the bedside making discharge decisions, clinical details are fresh. Document the hospital course in real time as you round on patients instead of reconstructing events hours later from memory and scattered notes.
Set team-wide completion expectations. When everyone knows summaries should be done within four hours of discharge, it becomes the standard instead of an aspirational goal. Peer accountability drives consistency.
Front-load documentation throughout the hospital stay. Update problem lists daily. Record major decisions and procedure notes as they happen. By discharge day, you're assembling pieces instead of writing from scratch.
Batch similar tasks together. Dedicate specific time blocks for discharge paperwork instead of context-switching between patient care and documentation.
Template Design and Auto-Population Techniques
Templates cut data entry without sacrificing personalization. The key is knowing which elements to auto-populate and which require your clinical judgment.
Start with fields your EHR already knows: patient demographics, admission date, discharge date, and attending physician. These should never require manual entry. Pull forward patient vital sign measurements from the final 24 hours, active medication lists, and scheduled follow-up appointments already in the system.
Build dropdown menus for common discharge dispositions (home, skilled nursing facility, rehab), standard diet instructions, and activity restrictions. Templates handle repetitive elements efficiently. For frequent diagnoses in your specialty, create pre-written templates with inline prompts that guide what to include. A pneumonia template might read: "[Describe severity, oxygen requirements, and response to antibiotics]." This preserves narrative flow while reducing blank-page paralysis.
The best templates feel like structured notes, not fill-in-the-blank forms. They handle repetitive elements so you can focus writing energy on the unique clinical story that matters for the next provider.
Common Mistakes That Slow Down Discharge Summary Writing
Writing from memory doubles your documentation time. When you reconstruct a five-day hospital stay hours after discharge, you're piecing together fragments instead of referencing daily progress notes. The cognitive load slows you down and creates more errors.
Overwriting buries critical information. Including every single vital sign change or routine nursing note forces the receiving provider to hunt for what matters. Focus on clinical decision points and medication changes instead of minute-by-minute timelines.
Dense paragraph blocks without clear headers create scanning friction. Structure your summaries with distinct sections so readers can quickly locate pending labs, follow-up appointments, and management changes.
Waiting until end of shift guarantees slower completion. Mental fatigue at 7 PM means you'll spend 20 minutes on what would take 8 minutes at 10 AM when clinical details are still fresh and your focus is sharper.
Voice Dictation as a Speed Multiplier for Clinical Documentation
Documentation Method | Words Per Minute | Time for 600-Word Summary | Key Advantages | Common Drawbacks |
|---|---|---|---|---|
Traditional Typing | 40 WPM | 15 minutes | Familiar workflow, direct EHR entry | Slow, high cognitive load, requires workstation |
Voice Dictation (Real-Time) | 120-150 WPM | 4-5 minutes | 3-4x faster, hands-free, captures fresh details | Requires adoption of new tool, initial learning curve |
Delayed Documentation | 30-35 WPM | 17-20 minutes | None (purely habit-based) | Memory gaps, increased errors, 1.60% higher readmission risk per day |
Voice + Templates | 150+ WPM | 3-4 minutes | Fastest method, auto-populates routine fields | Requires initial template setup |
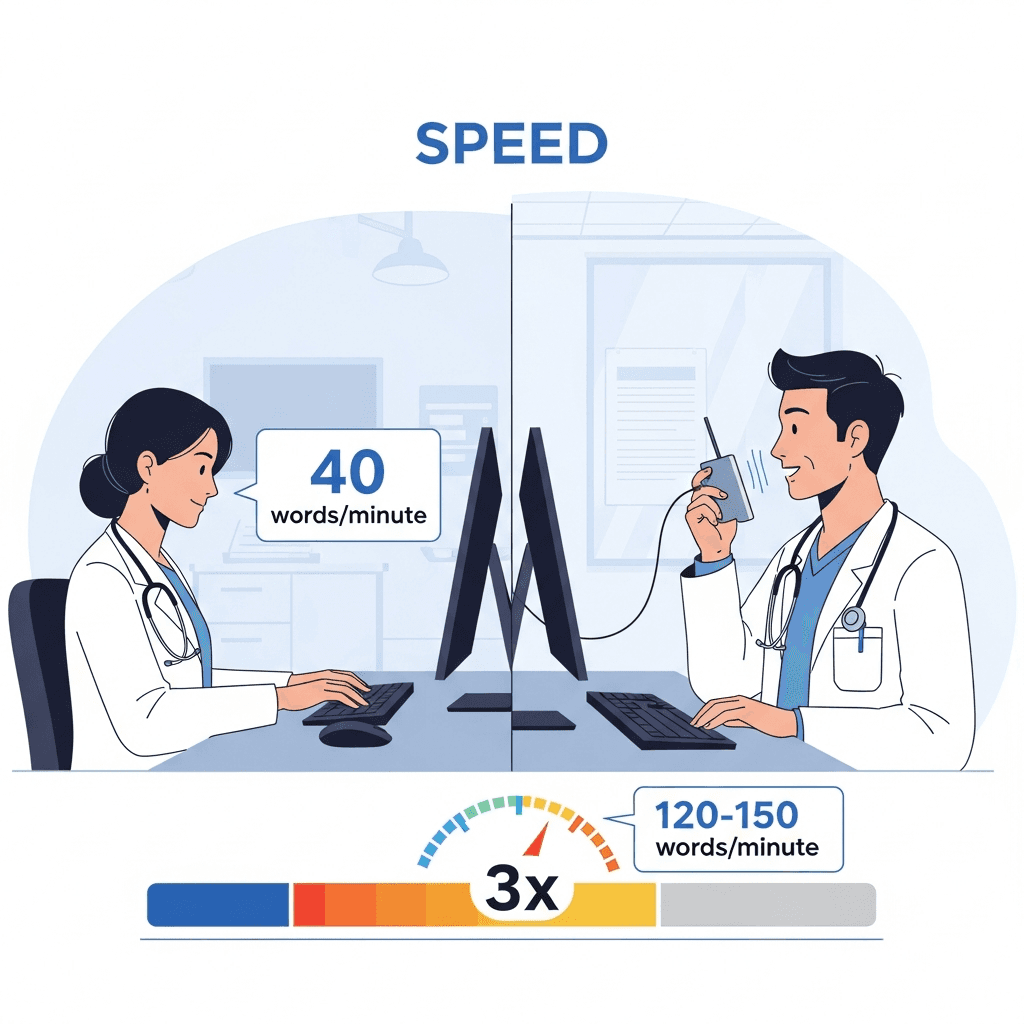
Speaking beats typing by a wide margin. You type around 40 words per minute. When you speak, you hit 120 to 150 words per minute. For narrative-heavy sections like hospital course descriptions, voice gives you a 3x to 4x speed advantage.
The benefit goes beyond raw speed. Speaking matches how you think. Clinical reasoning flows verbally, helping you maintain flow state while speaking. When you speak your notes, thoughts translate directly into words without the manual bottleneck of typing. Your brain isn't splitting attention between what happened to the patient and where your fingers need to go next.
Voice tools also allow physicians to document quickly during natural pauses in the workflow, such as immediately after rounds or while reviewing the chart. These small pockets of time add up when you can speak instead of needing to sit at a workstation with a keyboard.
For physicians already underwater with documentation, that 3x multiplier means finishing a 15-minute discharge summary in five minutes. The same speed advantage applies when using voice dictation for ChatGPT to draft complex clinical notes. Over a week, you get hours back.
How AI-Powered Voice Dictation Works for Physicians Using Willow
Willow turns dictation into clinical documentation by recording your voice and converting it to text in under 200 milliseconds. Press the function key, speak your hospital course narrative, and text appears faster than any other dictation tool. That speed keeps you in flow state instead of waiting for words to catch up.
The tool learns your medical vocabulary after the first correction. When you say "Dr. Patel" or "levofloxacin," it remembers the spelling and adds terms to your personal dictionary automatically, similar to how voice dictation for coding adapts to technical syntax. This personalization makes Willow more accurate for you over time, which means fewer edits to discharge summaries.
For protected health information, Willow maintains SOC 2 and HIPAA compliance with zero data retention. Teams get shared shortcuts and dictionary terms that speed up documentation across your group while keeping patient data private.
FAQs
What sections must every discharge summary include to meet standards?
You need patient demographics, admission details, a hospital course narrative, complete medication reconciliation with changes flagged, and specific follow-up instructions with any pending test results.
How much faster is voice dictation compared to typing for clinical documentation?
You can speak at 120-150 words per minute versus typing at 40 words per minute, giving you a 3x to 4x speed advantage for narrative sections like hospital course descriptions.
How does Willow protect patient health information during dictation?
Willow maintains SOC 2 and HIPAA compliance with zero data retention policies, processes your voice in under 200 milliseconds, and offers offline mode for completely local dictation when needed.
Final Thoughts on Improving Discharge Summary Completion
Improving discharge summary completion starts with changing when and how documentation happens. When physicians capture clinical reasoning during rounds and use voice dictation to record the hospital course at speaking speed, summaries that once took 15 to 20 minutes can take only a few minutes while details are still accurate. That approach sits at the core of how to streamline discharge summary writing: document while decisions are fresh, rely on structured templates, and reduce the time spent reconstructing events from memory after your shift. Tools like Willow support this workflow by converting spoken explanations into structured discharge summaries inside the systems clinicians already use, helping physicians complete documentation faster while maintaining clear records for the next provider in the care chain.
Physicians often spend 15 to 20 minutes writing each discharge summary, usually hours after rounds when key clinical details are harder to recall. That delay turns a straightforward documentation task into a slow reconstruction of decisions, medications, and follow-up plans from memory. Learning how to streamline discharge summary writing begins with capturing information while patient care is still unfolding and using voice-based documentation that records clinical reasoning at speaking speed. Instead of typing summaries long after discharge, clinicians can speak their hospital course and care plan while details are still fresh, turning real-time explanations into structured documentation inside the EHR with modern dictation software.
TLDR:
Delayed discharge summaries increase 30-day readmissions by 1.60% per day of delay.
Speaking reaches 120-150 words per minute versus 40 typing, cutting documentation time by 3-4x.
Complete summaries during rounds when clinical details are fresh, not hours later.
Templates and auto-populated EHR fields remove repetitive data entry from discharge summaries.
Some modern tools learn your medical vocabulary with 200ms speed and HIPAA compliance for team-wide documentation.
Why Discharge Summary Speed Matters for Patient Safety and Care Transitions
Discharge summaries go beyond documentation. When these documents are delayed or incomplete, patients face real risks during care transitions.
The numbers tell a concerning story. Research shows that 37.6% of discharge summaries are released at least one day after patients leave the hospital. For every day of delay, the likelihood of 30-day hospital readmission increases by 1.60%. Longer delays in completing discharge summaries are associated with higher rates of 30-day readmission in some studies.
These delays create dangerous information gaps. Primary care physicians receiving patients may lack critical details about medications changed during hospitalization, pending test results, or necessary follow-up appointments. Without this information, care coordination breaks down.
The consequences extend beyond readmissions. Incomplete summaries contribute to medication errors, duplicated tests, and missed diagnoses. When your next provider doesn't know what happened during your hospital stay, they're working blind.
Faster completion isn't about checking boxes. In the days following discharge, when patients are particularly vulnerable to complications, a complete summary can help prevent emergency visits and catch issues early.
The True Cost of Documentation Burden on Physicians
Documentation drains more than time. Physicians spend 15.5 hours weekly on paperwork and admin tasks, according to the 2023 Medscape Physician Compensation Report. Reducing documentation time becomes critical as these hours add up. That translates to nearly two full workdays diverted from patient care.
Those hours add up fast. At four patients per hour, 15.5 hours of admin work means 62 patients you could have seen each week. Over a year, that's more than 3,000 missed appointments per physician.
For physicians who could otherwise see patients during that time, administrative work represents a substantial opportunity cost in both patient access and clinical productivity. But the real toll isn't financial. Burnout rates climb as documentation demands grow. Time spent writing discharge summaries late at night is time away from family, sleep, and recovery.
You didn't train for a decade to become a data entry specialist.
Critical Components of an Effective Discharge Summary
Every discharge summary needs specific elements to meet Joint Commission standards and protect patients during transitions. The goal is completeness without bloat.
Patient Demographics and Admission Details
Start with the basics: patient name, medical record number, admission date, discharge date, and attending physician. Include the primary admission diagnosis and any secondary diagnoses that shaped the hospital course. Medical summaries require precision and completeness. These identifiers prevent confusion when multiple providers review the record.
Hospital Course Narrative
Summarize what happened during the stay in chronological order. Focus on clinical decision-making, procedures performed, and how the patient responded to treatment. Skip routine vital sign trends unless they informed major clinical decisions. This section answers: why did this patient need hospitalization, and what changed?
Medication Reconciliation
List all discharge medications with dosages, frequencies, and duration. The ability to speak medical terms without errors prevents dangerous transcription mistakes. Flag any changes from pre-admission medications. Note what was stopped, started, or adjusted. This prevents dangerous drug interactions and duplicate prescriptions.
Follow-Up and Pending Results
Specify which provider should see the patient, when, and why. Document any lab results or imaging studies still pending at discharge. Without this, critical findings fall through the cracks.
Workflow Optimization Strategies to Reduce Completion Time
Small process changes create big time savings. Quality improvement initiatives have reduced discharge summary completion time by 70%, dropping from 71.5 hours to just 21.8 hours. The secret isn't working harder, but restructuring when and how you document.
The most effective change? Complete summaries during rounds instead of after your shift ends, using professional dictation software to capture information in real time. When you're at the bedside making discharge decisions, clinical details are fresh. Document the hospital course in real time as you round on patients instead of reconstructing events hours later from memory and scattered notes.
Set team-wide completion expectations. When everyone knows summaries should be done within four hours of discharge, it becomes the standard instead of an aspirational goal. Peer accountability drives consistency.
Front-load documentation throughout the hospital stay. Update problem lists daily. Record major decisions and procedure notes as they happen. By discharge day, you're assembling pieces instead of writing from scratch.
Batch similar tasks together. Dedicate specific time blocks for discharge paperwork instead of context-switching between patient care and documentation.
Template Design and Auto-Population Techniques
Templates cut data entry without sacrificing personalization. The key is knowing which elements to auto-populate and which require your clinical judgment.
Start with fields your EHR already knows: patient demographics, admission date, discharge date, and attending physician. These should never require manual entry. Pull forward patient vital sign measurements from the final 24 hours, active medication lists, and scheduled follow-up appointments already in the system.
Build dropdown menus for common discharge dispositions (home, skilled nursing facility, rehab), standard diet instructions, and activity restrictions. Templates handle repetitive elements efficiently. For frequent diagnoses in your specialty, create pre-written templates with inline prompts that guide what to include. A pneumonia template might read: "[Describe severity, oxygen requirements, and response to antibiotics]." This preserves narrative flow while reducing blank-page paralysis.
The best templates feel like structured notes, not fill-in-the-blank forms. They handle repetitive elements so you can focus writing energy on the unique clinical story that matters for the next provider.
Common Mistakes That Slow Down Discharge Summary Writing
Writing from memory doubles your documentation time. When you reconstruct a five-day hospital stay hours after discharge, you're piecing together fragments instead of referencing daily progress notes. The cognitive load slows you down and creates more errors.
Overwriting buries critical information. Including every single vital sign change or routine nursing note forces the receiving provider to hunt for what matters. Focus on clinical decision points and medication changes instead of minute-by-minute timelines.
Dense paragraph blocks without clear headers create scanning friction. Structure your summaries with distinct sections so readers can quickly locate pending labs, follow-up appointments, and management changes.
Waiting until end of shift guarantees slower completion. Mental fatigue at 7 PM means you'll spend 20 minutes on what would take 8 minutes at 10 AM when clinical details are still fresh and your focus is sharper.
Voice Dictation as a Speed Multiplier for Clinical Documentation
Documentation Method | Words Per Minute | Time for 600-Word Summary | Key Advantages | Common Drawbacks |
|---|---|---|---|---|
Traditional Typing | 40 WPM | 15 minutes | Familiar workflow, direct EHR entry | Slow, high cognitive load, requires workstation |
Voice Dictation (Real-Time) | 120-150 WPM | 4-5 minutes | 3-4x faster, hands-free, captures fresh details | Requires adoption of new tool, initial learning curve |
Delayed Documentation | 30-35 WPM | 17-20 minutes | None (purely habit-based) | Memory gaps, increased errors, 1.60% higher readmission risk per day |
Voice + Templates | 150+ WPM | 3-4 minutes | Fastest method, auto-populates routine fields | Requires initial template setup |
Speaking beats typing by a wide margin. You type around 40 words per minute. When you speak, you hit 120 to 150 words per minute. For narrative-heavy sections like hospital course descriptions, voice gives you a 3x to 4x speed advantage.
The benefit goes beyond raw speed. Speaking matches how you think. Clinical reasoning flows verbally, helping you maintain flow state while speaking. When you speak your notes, thoughts translate directly into words without the manual bottleneck of typing. Your brain isn't splitting attention between what happened to the patient and where your fingers need to go next.
Voice tools also allow physicians to document quickly during natural pauses in the workflow, such as immediately after rounds or while reviewing the chart. These small pockets of time add up when you can speak instead of needing to sit at a workstation with a keyboard.
For physicians already underwater with documentation, that 3x multiplier means finishing a 15-minute discharge summary in five minutes. The same speed advantage applies when using voice dictation for ChatGPT to draft complex clinical notes. Over a week, you get hours back.
How AI-Powered Voice Dictation Works for Physicians Using Willow
Willow turns dictation into clinical documentation by recording your voice and converting it to text in under 200 milliseconds. Press the function key, speak your hospital course narrative, and text appears faster than any other dictation tool. That speed keeps you in flow state instead of waiting for words to catch up.
The tool learns your medical vocabulary after the first correction. When you say "Dr. Patel" or "levofloxacin," it remembers the spelling and adds terms to your personal dictionary automatically, similar to how voice dictation for coding adapts to technical syntax. This personalization makes Willow more accurate for you over time, which means fewer edits to discharge summaries.
For protected health information, Willow maintains SOC 2 and HIPAA compliance with zero data retention. Teams get shared shortcuts and dictionary terms that speed up documentation across your group while keeping patient data private.
FAQs
What sections must every discharge summary include to meet standards?
You need patient demographics, admission details, a hospital course narrative, complete medication reconciliation with changes flagged, and specific follow-up instructions with any pending test results.
How much faster is voice dictation compared to typing for clinical documentation?
You can speak at 120-150 words per minute versus typing at 40 words per minute, giving you a 3x to 4x speed advantage for narrative sections like hospital course descriptions.
How does Willow protect patient health information during dictation?
Willow maintains SOC 2 and HIPAA compliance with zero data retention policies, processes your voice in under 200 milliseconds, and offers offline mode for completely local dictation when needed.
Final Thoughts on Improving Discharge Summary Completion
Improving discharge summary completion starts with changing when and how documentation happens. When physicians capture clinical reasoning during rounds and use voice dictation to record the hospital course at speaking speed, summaries that once took 15 to 20 minutes can take only a few minutes while details are still accurate. That approach sits at the core of how to streamline discharge summary writing: document while decisions are fresh, rely on structured templates, and reduce the time spent reconstructing events from memory after your shift. Tools like Willow support this workflow by converting spoken explanations into structured discharge summaries inside the systems clinicians already use, helping physicians complete documentation faster while maintaining clear records for the next provider in the care chain.

Try Willow for free
Instant, accurate voice dictation. No card required.
Try Willow for free
Instant, accurate voice dictation. No card required.
Other stories you’ll love
Other stories you’ll love


Your keyboard is optional now
" transform="translate(5 5)" width="9.791000051498413px"/></svg>)

The voice-first interface for modern work.
© Willow Care, Inc. 2026. All rights reserved
Your keyboard is optional now
The voice-first interface for modern work.
© Willow Care, Inc. 2026. All rights reserved
Your keyboard is optional now
The voice-first interface for modern work.
© Willow Care, Inc. 2026. All rights reserved